***Updated December 31, 2021 - now with better writing, and discussion of the racial disparities in diabetes diagnoses. Many thanks to Mandy for correcting my broad-stroked (and sometimes incorrect) medical claims***
I sat down to consider if government-imposed vaccine passports are a violation of one’s freedom, specifically in the context of the COVID-19 pandemic. I live in an affluent country that was first in line to receive vaccines; my mother recently received her third dose, and I’m booked to receive mine in February 2022. The personal choice to refuse vaccination has become a point of contention in the global north, overshadowing the calls to unity that began this pandemic. However, there is a large gap in who can consider refusing vaccination. In this paper, I explore how to best support the goal of public health while respecting autonomy, borrowing rationales from modern libertarian thinkers to give these arguments a broader appeal.
I find it futile to place focus on individual dissenters during a pandemic and expose the long-term risks of relying on herd immunity. Instead, it is of greater importance to increase worldwide access to vaccines, and the interdependent nature of human health motivates the capabilities approach as discussed by Martha Nussbaum. With some adjustments, I believe that similar arguments can be made for other capabilities such as housing and food security—that it is in everyone’s self-interest to ensure these capabilities for others—but that is beyond the scope of this paper. I begin with a justification of vaccine uptake with a passport system in the global north before broadening to a discussion of epidemiology and vaccine distribution.
The distribution systems created during this pandemic are inherently undemocratic as they rest on and reaffirm colonial power imbalances. Therefore, I will end by offering suggestions for wealth distribution and the funding of healthcare in the global south to disrupt the impact of these deep-rooted fissures in future global pandemics.
Specifications
There are real and measurable risks to having many unvaccinated people during a global pandemic. They portend large outbreaks, and those losses cascade into diminished public trust (in vaccines, each other, and the government); economic losses from closures; and sickness or death (Navin, 2015, p. 175).
In my appeals to the unvaccinated, I am not targeting large pockets without access to vaccines nor those who face barriers to receiving them, all of whom can be aided through greater communication and the democratic access to healthcare I’ll discuss below. I’m focused on those in the global north who have vaccines readily available and intentionally choose not to take them. For this paper, I use the global north to describe the beneficiaries of colonialism, and the global south to indicate where wealth continues to be extracted from. (Simoes, 2021). This paper endorses a vaccine passport system (that must not be easily falsifiable) in all countries with enough vaccines for their population. This passport system limits access to public amenities such as restaurants, events, and schools. I will discuss exceptions, complications, and calls for further thought below.
False Start & Capabilities
A common argument for vaccine uptake is that we conventionally accept pre-emptive coercion when the harm is serious and the coercion reduces the risk of harm without serious side effects (Navin, 2015, p. 174). While this applies to levels of coercion such as seatbelts and the carrying of weapons, it doesn’t intuitively apply to injecting a foreign substance into oneself, which may cause side effects. Another reason arguments like this fail is because there are plenty of people who do not accept such coercion, and choose to freely drive without seatbelts and carry concealed firearms, because it’s ‘their risk to take on’. Paternalistic mandates implemented in citizens’ ‘best interest’ are ultimately externally motivated, which will fail on those who are sensitive to authority and want to make free, informed choices. Instead, there is more value in motivating vaccine acceptance from the inside: where it is purely in one’s self-interest to receive the vaccine.
In Women and Human Development, philosopher Martha Nussbaum discusses the capabilities approach, which lists essentials to ensuring a quality of life that is worthy of human dignity (2001, p. 73). The capabilities approach asks us to consider what someone is capable of doing. Does a person have the capability to move freely, or enjoy a long life with good health? To fulfil these, social systems and institutions are required, and as such, the ideal way to fulfil these capabilities uses both “practical reason and affiliation” (2001, p. 82). Community is required for fulfilling these capabilities from the production or movement of goods to the simple cognitive benefits of affiliation with others (Nussbaum, 2001, p. 79). In his work on institutional fairness under capitalism, Waheed Hussain further remarks on the importance of community. Both authors comment that some amount of care for the people around you is important in a functioning community, and can be employed as a form of power against institutions that may not have one’s interests as their priority (Hussain, 2020, p. 79; Nussbaum, 2001, p. 79). T
Though we can motivate the uptake of vaccines on the grounds of “care for others in a healthy community”, there will always be those who are not moved by this argument and require a purely self-interested motivation, as perhaps they would be happy living largely in isolation. However, the importance of community can motivate in a purely self-interested way, where one performs a role within the constraints of the community to have needs met.
For this, we turn to feminist scholar Uma Narayan’s (2002) concept of the ‘bundle of elements’. In Minds of Their Own, Narayan discusses that the choice to wear religious garments should not be seen as inherently oppressive, but instead a method of bargaining within the constraints of society to have needs met (2002, pp. 420-421). To meet our needs, there are sacrifices we make for the sole reason that we require other people to meet them. Just as some may wear religious garments or adhere to standards of gender expression to feel safe and accepted in their community, everyone makes sacrifices in public institutions in which community member roles must be performed. We sacrifice money to purchase goods; time to work or wait in line; individuality in institutions that demand conformity (like the army or school); and it follows that we must maintain basic conventions of hygiene to protect the health of others in order to gain the conveniences of their presence.
The constraints of society result from choices made in the past that we cannot negotiate with now, but that does not make these choices unfree, because they have significant stakes to the people that make them (Narayan, 2002, p. 422). In a world that is rapidly spreading diseases through warming and globalization, we have reached the inevitable inclusion of vaccines for those who want to best maintain their health while receiving the benefits of a community. We can imagine this bundle holding both a vaccine and a passport to public amenities. The choice can be made to take the bundle or not, the consequence of which is the loss of amenities, but importantly not the ones needed to live such as grocery stores and clinics, which would correctly spur the retort of the loss of resources for living.
Libertarian Freedom & Complications
As libertarian thinkers hold that freedom is the most important value, my aim in using their ideology to motivate arguments mirrors the project of philosopher Jason Brennan—the libertarian’s emphasis on personal autonomy appears to “load the dice” against the governmental imposition of anything (2016, p. 37). Therefore, if the following claims can be justified through this ideology, they likely will appeal to a broad group of thinkers who value freedom.
In response to government-imposed shutdowns, American conservative Matthew Parris made an argument akin to Narayan’s bundles: that the passport system aimsto increase liberty by restricting optional spaces to those who will not be put at risk, as an alternative to shutting those spaces down (2021). This increases liberty among the vaccinated, creating a net benefit over complete closure. Future freedoms are also protected, as higher rates of sickness increase possibilities that the production and sales of essentials will stop or become prohibitively expensive, limiting their availability. In a global market, this potentially spells disaster for availability in the global south, and among the working class of the north, both of whom will be pressured to work in these dangerous environments through the loss of emergency benefits, and rhetoric of ‘laziness’ (Swift & Power, 2021).
As a result of expressing one’s freedom to make choices, the consequences must also be accepted, which makes moral responsibility a focus of libertarians (Brennan, 2017, p. 40). Instead of being a tightly organized group, Brennan specifies ‘anti-vaxxers’ as “people who actively chose to behave in certain reckless ways, rather than…people who simply failed to choose to behave in certain publicly beneficial ways” (Brennan, 2017, p. 41). He notes that those who choose not to vaccinate put in the epistemic effort to rationalize their decisions, as informed apathy would look like following medical experts (2017, p. 40). To justify exposing another party to a risk, Brennan further argues that it must be part of an equitable social system of risk-taking that offers an advantage to the other party involved (Brennan, 2017, pp. 40-41). Since there is no clear benefit offered to the vaccinated to have the unvaccinated mingling about—it is a self-involved interest that shirks personal responsibility. From this, he argues that this group can be justifiably prohibited from participating in the collective imposition of unjust risk of harm to others (Brennan, 2017, p. 42).
Stronger libertarians may further disagree, arguing that individual businesses ought to have a say in whether they will serve the unvaccinated. This type of argument fits into the risk relationship as the business does gain patronage as a result of being exposed to the risk of contracting the disease. As well, other customers potentially benefit because the increased business may keep the store open during the pandemic or expand their selection. Arguments against this will have to develop some threshold of risk that the public can justifiably be exposed to in conversation with the potential benefits. In action, this could look like having signs informing the vaccinated that they are allowing the unvaccinated inside–thereby allowing patrons to decide if they will continue visiting–allowing the fate of the establishment to the passions of the market.
A Note on ‘My Body, My Choice’
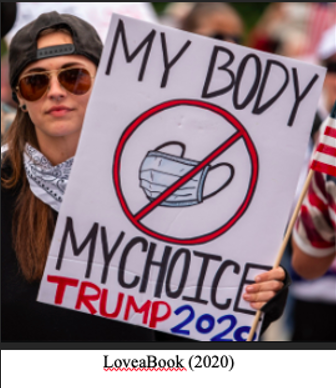
This feminist argument is being cleverly deployed by the anti-vaccination community. Its original stance lies in granting individuals the ability to choose what they can do with their bodies against oppressive forces that were denying them medical treatment. While the words appeal to the message of choosing what goes into their body, users also—possibly unintentionally—invoke the original role of the message, which was to increase overall capabilities by increasing access to medical care for women. Following through in this case would look like an increase in global vaccine administration, which will likely remove resources and focus from coercing skeptics, who may become less skeptical as the vaccine does its job and slows the proliferation of new variants.
Preconditions for Skepticism
‘Should I get the vaccine?’
The question above is the manifestation of northern worries about personal freedom; one that a very small amount of the earth’s population has the opportunity to consider right now. The intense focus, emotional commentary, and dramatization of this individual choice conceals the true lack of freedom within this pandemic, which is the starkly different realities in the global north and south. Readily available vaccines allow for the luxury of doubting medical professionals who have spent their lives preparing for these disasters because there appears to currently be a relatively small risk in doing so. Jamaica Kincaid wrote of similar preconditions for epistemic thought in Autobiography of my Mother:
A man proud of the pale hue of his skin cherishes it especially because…he was born that way…and it gives him a special privilege in the hierarchy of everything…What makes the world turn is a question he asks when all that he can see is securely in his grasp, so securely in his grasp that he can cease to look at it from time to time, he can denounce it (2013, p.131).
Descartes was able to sit in his chair and doubt his body because it didn’t inform the shape of his life, but those who looked different and were sold to him in servitude didn’t have the luxury of philosophical thought. We see this power dynamic played out in vaccine hesitancy: having the preconditions to doubt something requires a) having it securely available, and b) (believed) social stability and security to abstract from. Both are present where skeptics live, and largely upset in the global south. I make the distinction of ‘believed’ social stability and security because in the global north this is largely an illusion, as media production norms and algorithms shield dissenters from the gruesome realities in other countries, and the contagious nature of the virus keeps northern news crews from hospitals (Smith, 2021). Those born in the global north through random chance can make the epistemic effort to rationalize refusing a vaccine for a pandemic with over five million victims because they can’t see the victims. The hesitant hold the benefits of colonialism to abstract from, which are inherited attitudes regarding what ‘counts’ as a community.
The Global Community
The longer that focus remains on individual choices, the further the lens blurs out larger conceptions of community. With the focus on individuals, the concept of community is purposefully kept narrow—never to include nearby countries, let alone the entire world. However, viruses do not operate under this myopic lens. The longer that anyone in the world goes without vaccines, the more mutations will emerge, leading to more pathogenic and virulent variants, which we’ve already seen with Delta and Omicron respectively. Instead of protecting public health, coercing individuals diverts attention and resources from increasing the availability of vaccines. We must consider the difference between choosing not to get an available vaccine, and not having that consideration due to lack of availability; the latter being the true threat to public health (Nussbaum, 2001, p. 84).
As of December 2021, The Bloomberg Vaccine Tracker notes that the least wealthy 52 places which hold 20.5% of the world’s population have 5.6% of the available vaccinations (Bloomberg, 2021). At our current vaccination rate, the Tracker estimates it will take three months until 75% of the earth’s population receives at least one dose (Bloomberg, 2021). Dr Leong Hoe Nam, a Singapore-based infectious disease doctor is predicting that within 3-6 months, the Omicron strain will have “overwhelmed” the world, and our best bet is an additional three doses of vaccines (Ng, 2021). It was also a few days shy of exactly three months between the emergence of Delta and Omicron variants, so if we continue our current vaccination schedule, it is likely we will be choosing between the names Sigma or Upsilon by spring 2022 (CDC, 2021). To the skeptics that retort “my health is only my responsibility,” they undermine their argument of personal responsibility by ignoring that viruses do not prescribe to our ideas of community–human health is interdependent to each other, other species, and the planet.
Casting our sights beyond the COVID-19 pandemic, we can consider the future of the ‘anti-vaxxer’ given current virologist predictions. There will inevitably be people in every country who refuse to become vaccinated for personal reasons. Given our current state of global warming, it is likely that we may soon see revivals of smallpox, spanish flu, anthrax, and other viruses contained in the burial grounds beneath the melting ice caps (McKenna, 2017). If not, the global north will eventually become susceptible to diseases that travel by mosquito or thrive in warm climates such as malaria, cholera, zika, and dengue fever, likely adding new vaccines to the list required of school-age children. (McKenna, 2017). With the variety of deadly viruses being introduced, herd immunity will quickly fail individuals who choose not to vaccinate, so it is truly in the best interest of vaccine skeptics to become part of the herd. There is a linguistic issue in using the ‘herd’ to describe where one would be safe, while the sheep is often symbolically weaponized as a mindless follower. For the age of pandemics, I propose that we instead appeal to our liberty-loving friends and describe this as a global fight for our freedom: away from illness and toward health, which allows for longer, freer lives.
Everyone’s freedom to live a healthy life is potentially impacted by not having COVID-19 vaccines available to all, which is truly a failure of not having a centralized democratic vaccine distribution system. Our current system required mass amounts of capital to create vaccines, which was supplied by resource-wealthy countries, placing them at the top of the list to receive doses. This system exposes the flaw in global market logic: it ignores the extractive-colonial roots of wealth, and inherently prioritizes the wealthy.
Colonialism’s Legacy on ‘Public’ Health
This pandemic has been a test run for global vaccination which has failed due to inequity rooted in colonialism. While this is being referred to as the ‘pandemic of the unvaccinated’, the vast differences between countries in vaccination rates are directly due to availability. A history of mining the global south for resources allowed the north to front the cost for vaccines, and therefore market logic dictates that they receive priority access. This recreates and emphasizes the current power imbalances, as the global south lacks the power to demand equitable access to vaccines.
Democratizing vaccine availability would disrupt these current power conditions, so focusing on the rhetoric of personal choice has the added benefit of making vaccination a personal issue instead of a global-political critique of the wealth legacy of colonialism. This pandemic has offered an opportunity for wealth redistribution from rich countries to amend the power relations between the global north and south, recognizing our shared humanity in the face of this virus. However, the global south is being held at the mercy of the north as the UN pleads for donations from northern stockpiles (2021).
Many countries, like Canada, are meeting their donation targets to the distributor COVAX with massive donations of the AstraZeneca vaccine, whose use has been suspended in much of the global north while the side effects are being investigated (Dean & Schuster-Bruce, 2021; Zimonjic, 2021; COVAX, 2021). Over half of Canada’s current contributions to COVAX have been of the AstraZeneca vaccine, which is now being shipped from manufacturers directly to the global south (Government of Canada, 2021). This donation of the potentially dangerous leftovers to the global south is only rational from the white supremacist’s mind—either the vaccines will work, or the side effects are of little importance to ‘those’ populations (Kashyap, 2020). It shows a blatant disregard for the global community, and a disturbing pattern of ‘othering’ once paired with the news of a Saugeen First Nation community being given expired doses of the vaccine for an entire month (Dubinsky, 2021). When someone is seen as the ‘other’, two roads can lead to the end of a pandemic: mass vaccination or mass extermination.
Recommendations & Conclusions
In 2009, Larry Brilliant of the Wall Street Journal noted that we were living in ‘The Age of Pandemics,’ discussing the then-current swine flu epidemic. The rationale for this naming comes from anthropogenic global warming (fewer ice barriers between countries, increased economic and climate migrants, and more diseases thriving in warm environments); globalizing technology leading to greater communication and migration; and increased meat consumption (Brilliant, 2009).
The forced implementation of extractive capitalism resembles a virus, against the systems in place that aimed for health and harmony with the earth. The exploitation, exclusion, and elimination of indigenous, black, and migrant populations leave them specifically vulnerable to respiratory diseases like COVID-19 (Kashyap, 2020). Historical and structural inequities have led to even greater vulnerability, with populations lacking running water and therefore unable to comply with handwashing recommendations (Kashyap, 2020).
This virus has specific targets: attaching to ACE2 receptors, those with diabetes or a family history of diabetes are especially susceptible (Scialo et al., 2020). This will target indigenous, black, and migrant populations who have a disproportionately high rate of diabetes, and likely higher rates of untreated diabetes due to lack of adequate healthcare (Kashyap, 2020). When these rates were noticed in the sixties, bio-logic was implemented, naming and blaming the tone-deaf ‘thrifty gene’ that supposedly slowed one’s metabolism as a result of a history of famine (O’Dea, 1995, p. 339). Newer research has linked the forced implementation of a colonial lifestyle as a multifaceted contributor to increased insulin resistance and weight gain (O’Dea, 1995, p. 340).
Diabetes, which had not existed for many of these populations, quickly became prevalent alongside the shift from wild foods to heavily processed (for both economic and safety reasons, as waters became polluted); enforced sedentary lifestyles; and the systems of work and currency that left little time or importance in home crops (Krotz, 2016).
Focusing on coercing individual choices is futile and ultimately unsuccessful at promoting public health. Instead, the focus ought to lie in thinking as a collective whole, understanding the history leading to our current conditions. Countries in the north must amend these imbalances and offer resources to redistribute wealth among the project of public health. Vaccines should be distributed by need, population density, and susceptibility. The project of human health expands beyond pandemics, as any country’s health relies on the health of all other countries. We may be able to prevent the future pandemics we know are coming by increasing the availability of both vaccines and adequate healthcare. The legacy of colonialism poses enormous threats to human health and wellbeing by withholding or providing sub-par healthcare to many populations. As the world continues to warm there will be more global pandemics, and leaving those in the global south to die might seem like an easy choice to the white supremacist’s mind. Even viewed through a callous, self-interested lens, inaction creates higher virus proliferation, summoning an impending and unavoidable threat.
Here we come to the contradiction of personal autonomy within public health: we can best support individual autonomy as a group. The experience of ourselves as a ‘self’ can only happen because we experience the existence of life that is not ourselves, and our interdependent existence against a global virus requires teamwork for the freedom of any one person to be ensured.
For the herd of humanity to survive this age of pandemics, we must remove the negative associations and remember the true value of the herd: access to community and a higher likelihood of survival. All of this considered, it is in any particular person’s interest for the sake of their freedom and life to participate in public health measures, just as it is rational to exclude those who make the epistemic effort to rationalize endangering themselves and others. Conceptions of community must be extended to include the global community, and the global north must develop healthcare in the global south, or find more room, infrastructure, and care for herd members from the global south to promote its own goals of health. To face a foe of our caliber, we must amend outdated power imbalances and recognize the interdependent nature of health across all life.
Reference List
Brennan, J. (2017, December 18). A libertarian case for mandatory vaccination. Journal of Medicine Ethics 44. 37-43. https://jme-bmjcom.myaccess.library.utoronto.ca/content/44/1/37.info
Brilliant, L. (2009, May 2). The Age of Pandemics. The Wall Street Journal. https:// http://www.wsj.com/articles/SB124121965740478983
Bloomberg. (2021, December 12). More Than 8.45 Billion Shots Given: Covid-19 Tracker. Bloomberg. Accessed December 13: https://www.bloomberg.com/graphics/covid- vaccine-tracker-global-distribution/
CDC. (2021, Dec 11). Omicron Variant: What You Need to Know. Centre for Disease Control and Prevention. https://www.cdc.gov/coronavirus/2019-ncov/variants/omicron- variant.html
COVAX. (2021, February 3). The covax facility: interim distribution forecast. From: https:// http://www.gavi.org/sites/default/files/covid/covax/COVAX-Interim-Distribution-Forecast.pdf
Dean, G., & Schuster-Bruce, C. (2021, March 16). Sweden joins Germany, France, and 15 other countries in suspending AstraZeneca’s vaccine over possible side effects. Business Insider. https://www.businessinsider.com/astrazeneca-covid-vaccine-countries-suspend- denmark-thailand-batch-blood-clots-2021-3?op=1
Dubinsky, K. (2021, September 24). Dozens of members of Saugeen First Nation in Ontario were given expired COVID-19 vaccines for a month. CBC. https://www.cbc.ca/news/ canada/London/saugeen-first-nation-expired-pfizer-vaccine-doses-1.6188281
Government of Canada. (2021, December 21). Canada’s international vaccine donations. Government of Canada. https://www.international.gc.ca/world-monde/issues_developmentenjeux_developpement/global_health-sante_mondiale/vaccine_donations-dons_vaccins.aspx?lang=eng
Hussain, W. (2020). Pitting People against each other. Philosophy & Public Affairs 48(1). Pp. 79-133
Kincaid, J. (2013). Autobiography of My Mother. Farrar, Straus & Giroux. Pp. 131-133.
Krotz, L. (2016, July 4). The link between diabetes among Indigenous peoples and colonialism. Broadview. https://broadview.org/the-link-between-diabetes-among-indigenous-peoples-and-colonialism/
Kashyap, M. K. (2020, November). U.S. Settler Colonialism, White Supremacy, and the Racially Disparate Impacts of COVID-19. California Law Review. https://www.californialawreview.org/settler-colonialism-white-supremacy-covid-19/#clr-toc-heading-1
LoveaBook. (2020, April 21). [online forum post] The irony in some of the protest signs is too rich! Reddit. Stable link: https://web.archive.org/web/20211230160031/https://www.reddit.com/r/TrollXChromosomes/comments/g5pd05/the_irony_in_some_of_these_protest_signs_is_too/
McKenna, J. (2017, May 11). The deadly diseases being released as ice thaws. World Economic Forum. https://www.weforum.org/agenda/2017/05/the-deadly-diseases-being-released- by-climate-change/
McKinnon, C. (2016). Should We Tolerate Climate Change Denial. Midwest Studies In Philosophy, XL
Narayan, U. (2002). Minds of Their Own: Choices, Autonomy, Cultural Practices, and Other Women in A Mind of One’s Own. eds. Antony, L. M. & Witt, C. E. pp. 418-432. https:// doi.org/10.4324/9780429502682
Navin, M. (2015). Values and Vaccine Refusal: Hard Questions in Ethics, Epistemology, and Health Care (1st ed.). Routledge. https://doi-org.myaccess.library.utoronto.ca/ 10.4324/9781315764078
Ng, A. (2021, December 2). Omicron will likely ‘dominate and overwhelm’ the world in 3-6 months, doctor says. CNBC. https://www.cnbc.com/2021/12/02/omicron-to-dominate- and-overwhelm-the-world-in-3-6-months-doctor-says.html
Nussbaum, M. (2001). Women and Human Development. Cambridge University Press. Pp 70-86.
O’Dea, K. (1995). Overview of the thrifty genotype hypothesis. Asia Pacific Journal of Clinical Nutrition 4(4). Pp. 339-40.
Parris, M. (2021, April 10). The libertarian case for vaccine passports. Spectator, 345(10050), 21. https://link.gale.com/apps/doc/A658442862/BIC?u=utoronto_main&sid=bookmark- BIC&xid=a8fe9579
Scialo, F., Daniele, A., Amato, F., Pastore, L. Matera, M. G., Cazzola, M., Castaldo, G., & Bianco, A. (2020). ACE2: The Major Cell Entry Receptor for SARS-CoV-2. Lung, 198(6). Pp. 867-877. https://doi.org/10.1007/s00408-020-00408-4
Simoes, V. (2021, September 20). Neocolonialism and the Global South. The Daily. https:// www.dailyuw.com/opinion/critical_conversations/neocolonialism-and-the-global-south- the-changes-and-recycling-of-colonialism/article_57330e42-2189-11ec- a49e-63739001b0b4.html
Smith, D. (2021, November 18). ‘We were in a war’: behind 2021’s most devastating Covid-19 documentary. The Guardian. https://www.theguardian.com/film/2021/nov/18/we-were-in-a-war-behind-2021s-most-devastating-covid-19-documentary
Swift, J, & Power, E. (2021, April 30). How COVID-19 and CERB proved that basic income is not only possible—it works. Canadian Dimension. https://canadiandimension.com/articles/view/how-covid-19-and-cerb-proved-basic-income-is-not-only-possible-it-works
UN. (2021, April 16). Unequal Vaccine Distribution Self-Defeating, World Health Organization Chief Tells Economic and Social Council’s Special Ministerial Meeting. United Nations. https:// www.un.org/press/en/2021/ecosoc7039.doc.htm
Zimonjic, P. (2021, July 12). Canada to donate almost 18 million surplus AstraZeneca doses to low- and middle-income countries. CBC. https://www.cbc.ca/news/politics/covax- donations-astrazeneca-surplus-1.6099072
